")
")

Genetic Research
 Family studies and studies on twins have clearly shown that both psoriasis and psoriatic arthritis have a great genetic component. People with a fist degree relative suffering from psoriasis are much more likely to start suffering from the disease if compared to the general population. In particular, the risk of psoriasis in patients’ children is 4 to 10 times higher. Studies on twins have shown a 62-70% consistency between monozygotic twins with respect to 21-23% of dizygotic twins. The mechanism of transmission of these diseases is apparently linked to many factors and the risk of a recurrence of PsA seems much higher compared to that of psoriasis. The risk of recurrence in a person with a first-degree relative suffering from psoriasis or Psoriatic Arthritis is 7.6 for the former and 30.4 for the latter. These data confirm the great importance of the genetic component behind the pathogenesis of these diseases. Many complex studies are required to understand exactly the genetic components behind these diseases.
Family studies and studies on twins have clearly shown that both psoriasis and psoriatic arthritis have a great genetic component. People with a fist degree relative suffering from psoriasis are much more likely to start suffering from the disease if compared to the general population. In particular, the risk of psoriasis in patients’ children is 4 to 10 times higher. Studies on twins have shown a 62-70% consistency between monozygotic twins with respect to 21-23% of dizygotic twins. The mechanism of transmission of these diseases is apparently linked to many factors and the risk of a recurrence of PsA seems much higher compared to that of psoriasis. The risk of recurrence in a person with a first-degree relative suffering from psoriasis or Psoriatic Arthritis is 7.6 for the former and 30.4 for the latter. These data confirm the great importance of the genetic component behind the pathogenesis of these diseases. Many complex studies are required to understand exactly the genetic components behind these diseases.
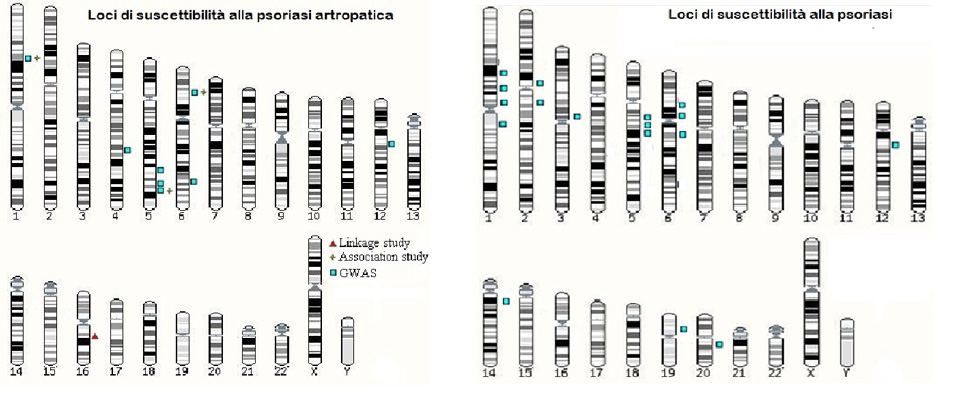
Many research groups have focused in these years on psoriasis and have highlighted many different psoriasis susceptibility loci (PSORS), i.e. DNA points capable of influencing directly or indirectly the development of the disease. Among the loci associated with psoriasis, there are: PSORS1 on the short arm of chromosome 6 (6p21.3), PSORS2 on the long arm of chromosome 17 (17q), PSORS4 on the long arm of chromosome 1 (1q21.3), PSORS5 on the long arm of chromosome 3 (3q21), PSORS6 on the short arm of chromosome 19 (19p), PSORS7 on the short arm of chromosome 1 (1p), PSORS8 on the long arm of chromosome 16 (16q), PSORS9 on the long arm of chromosome 4 (4q28-32) and PSORS10 on the short arm of chromosome 18 (18p11). The presence of all these loci is evidence of the great amount of studies made to discover them, but if we actually investigate their weight on influencing the risk to develop psoriasis, we will see it is very little. This makes us deduct that the role of genetics is linked to a great number of variables that, if taken singularly have little effect. This specific genetic scenario behind psoriasis does not allow us to establish a valid genetic test to define each individual risk.
For what concerns, psoriatic arthritis, we know a lot less about its genetic basis. Psoriasis and Psoriatic Arthritis are both associated with locus PSORS1, localised in chromosome 6 near the region responsible for codifying the greater system of histocompatibility. This region contains some of the most important genes responsible for immune response. The first evidence of the association between psoriasis and the HLA system were discovered in the 70s and then confirmed later on with the introduction of new techniques of analysis. The first genes to be identified were HLA-C, in particular HLA-Cw6 and HLA-B. Researchers then discovered that the association with HLA-B was merely due to a linkage disequilibrium with HLA-C. Linkage disequilibrium is the tendency that some genetic variants have to be inherited together. Significant associations were found also with PsA. In particular, whilst HLA-B*13, *16, *38, *39, *17 and HLA-Cw6 may have an effect on the onset of psoriasis (or of PsA), HLA-B*27 and *7 are specifically associated to PsA, and especially to those forms linked to an early onset of psoriasis.
 Great progress has been made in understanding the mechanisms behind psoriasis and psoriatic arthritis; many genetic and environmental factors have been identified and current medical treatments can take into account many different environmental factors. For what concerns genetic factors, we have seen that despite the many studies made, we still know very little. Currently identified loci can explain only a small fraction of the estimated inheritance, thus only a very little part of the risk due to the fact one has a first-degree relative suffering from the disease is linked to the presence/absence of oversensitivity/protection loci. In the near future, the progress of research and the introduction of new techniques capable of analysing not only genomic variants, but also epigenetic variants, will allow us to identify new factors and clarify the specific role of the factors we already know. Progress in the research on psoriasis and psoriatic arthritis will improve our knowledge on the origin of these diseases and help foresee the onset and development as well as one’s response to treatments. This could make us develop specific tailor-made treatments based on data that can be easily obtained, such as DNA and environmental factors to which the patients is exposed.
Great progress has been made in understanding the mechanisms behind psoriasis and psoriatic arthritis; many genetic and environmental factors have been identified and current medical treatments can take into account many different environmental factors. For what concerns genetic factors, we have seen that despite the many studies made, we still know very little. Currently identified loci can explain only a small fraction of the estimated inheritance, thus only a very little part of the risk due to the fact one has a first-degree relative suffering from the disease is linked to the presence/absence of oversensitivity/protection loci. In the near future, the progress of research and the introduction of new techniques capable of analysing not only genomic variants, but also epigenetic variants, will allow us to identify new factors and clarify the specific role of the factors we already know. Progress in the research on psoriasis and psoriatic arthritis will improve our knowledge on the origin of these diseases and help foresee the onset and development as well as one’s response to treatments. This could make us develop specific tailor-made treatments based on data that can be easily obtained, such as DNA and environmental factors to which the patients is exposed.
ADIPSO’S SUPPORT TO GENETIC RESEARCH
ADIPSO has always believed in genetic research and in the potentials of genetics as a tool to prevent and treat psoriasis. ADIPSO’s support to the research group headed by Prof. Giusepe Novelli of the University of Rome ‘Tor Vergata’ has allowed the group to carry out important genetic studies aimed at understanding the molecular basis of the disease. A very important discovery was the one that established that the region named 1q21 on chromosome 1 contains very important genes for the development of the disease. More specifically, we have seen that this region is fundamental in particular for Italian patients; this has established the basis for a personalised genetic medicine. Further studies financed by ADIPSO have identified the oversensitivity genes for psoriasis present on this chromosome. Great results have also been obtained to evaluate the genetic component of psoriatic arthritis. More specifically, all main genes involved have been identified through a great study that saw the participation/collaboration of the most important research groups on psoriasis at global level. Italy participated thanks to ADIPSO’s support.
